Critical Care Study Guide
ABG Interpretation Made Simple for Nurses
Learn a clean, repeatable approach to arterial blood gas interpretation with exam-style cases, compensation logic, and bedside context you can apply in class, clinicals, and NCLEX prep.
ABG basics and normal ranges
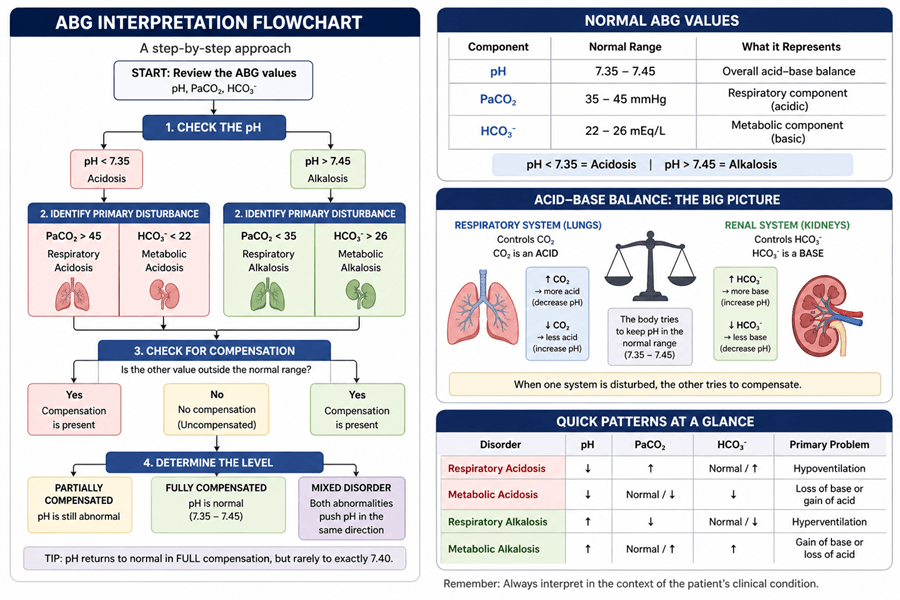
ABG interpretation becomes easier when you use a fixed order. Start by deciding if the patient is acidotic or alkalotic, then identify whether the respiratory or metabolic value explains that direction.
Memorize these core ranges before practicing case questions: pH 7.35-7.45, PaCO2 35-45 mmHg, HCO3 22-26 mEq/L.
The 4-step ABG method
Step 1: Read pH first
pH below 7.35 suggests acidosis. pH above 7.45 suggests alkalosis.
Step 2: Find the primary driver
If PaCO2 aligns with pH direction, think respiratory. If HCO3 aligns, think metabolic.
Step 3: Check for compensation
In metabolic disorders, lungs adjust CO2. In respiratory disorders, kidneys adjust bicarbonate.
Step 4: Classify compensation level
Uncompensated, partially compensated, or fully compensated based on pH and opposite-system movement.
Rapid interpretation checklist
- Classify pH as acidotic or alkalotic.
- Match pH change to PaCO2 or HCO3 to identify the primary disorder.
- Look at the opposite system for compensation.
- If pH is normal but values are abnormal, decide if compensation is full.
- If both PaCO2 and HCO3 push pH the same way, suspect a mixed disorder.
Reference patterns table
| Condition | pH | PaCO2 | HCO3 |
|---|---|---|---|
| Respiratory acidosis | ↓ | ↑ | Normal or ↑ |
| Respiratory alkalosis | ↑ | ↓ | Normal or ↓ |
| Metabolic acidosis | ↓ | Normal or ↓ | ↓ |
| Metabolic alkalosis | ↑ | Normal or ↑ | ↑ |
Practice cases with answers
Case 1
ABG: pH 7.32, PaCO2 50, HCO3 28
Answer: Partially compensated respiratory acidosis.
Case 2
ABG: pH 7.37, PaCO2 50, HCO3 30
Answer: Fully compensated respiratory acidosis.
Case 3
ABG: pH 7.10, PaCO2 60, HCO3 18
Answer: Mixed respiratory and metabolic acidosis.
Common mistakes to avoid
- Stopping after naming the primary disorder and skipping compensation.
- Assuming normal pH means no disorder.
- Ignoring mixed acid-base problems in very sick patients.
- Memorizing patterns without practice under timed conditions.
Related reading: Oxygen Therapy Guide and more NurseDive articles .
Build exam speed with NurseDive
If you want structured drills beyond this article, NurseDive has focused study paths for TEAS, nursing school success, and NCLEX prep.
TEAS Science Prep
Anatomy, physiology, and science walkthroughs built for score gains.
Nursing School Support
Med-surg concept maps and high-yield frameworks for class exams.
NCLEX Readiness
Priority questions, decision trees, and test strategy practice.
Frequently asked questions
What are normal ABG values for nurses to memorize?
Use this baseline: pH 7.35-7.45, PaCO2 35-45 mmHg, HCO3 22-26 mEq/L.
How do I tell respiratory from metabolic disorders on ABG?
Match the pH direction with the value moving in the same direction. CO2 points to respiratory causes and HCO3 points to metabolic causes.
Why can pH be normal even when ABG is abnormal?
A normal pH can happen in fully compensated disorders. CO2 and HCO3 may both be abnormal even if pH returns to the normal range.
References
Barnette L, Kautz DD. Creative ways to teach arterial blood gas interpretation. Dimensions of Critical Care Nursing. 2013;32(2):84-87.
Samuel R. A graphical tool for arterial blood gas interpretation using standard bicarbonate and base excess. Indian Journal of Medical Biochemistry. 2018;22(1):85-89.
Sood P, Paul G, Puri S. Interpretation of arterial blood gas. Indian Journal of Critical Care Medicine. 2010;14(2):57.
Williams AJ. Assessing and interpreting arterial blood gases and acid-base balance. BMJ. 1998;317(7167):1213-1216.
Verma AK, Roach P. The interpretation of arterial blood gases. Australian Prescriber. 2010;33(4):124-129.